

BACKGROUND
The phase 3 REACH2 trial (NCT02913261; N = 309) was the first successful randomized study in SR aGVHD, demonstrating that RUX, a JAK1/2 inhibitor, was superior to BAT. At day 28, RUX pts had a significantly higher overall response rate (ORR) than BAT pts (62.3% vs 39.4%; P < .001). RUX also led to a higher durable ORR at day 56 (39.6% vs 21.9%; P < .001) and showed clinically meaningful treatment benefits across pt subgroups of baseline characteristics; failure-free survival was longer with RUX (5.0 vs 1.0 month; HR, 0.46; 95% CI, 0.35 to 0.60) (Zeiser R, et al. NEJM. 2020).
The safety profile of RUX was as expected in pts with SR aGVHD, with cytopenias being the most common adverse events (AEs). To further define the safety profile of RUX in SR aGVHD, we report additional safety data up to day 28.
METHODS
Pts ≥ 12 years old with grade II-IV aGVHD following allogeneic hematopoietic cell transplant (alloHCT) who were refractory to steroids were randomized 1:1 to RUX (starting dose, 10 mg bid) or investigator-selected BAT and stratified by aGVHD grade. Crossover to RUX was allowed in BAT pts who had not responded by day 28 or lost response thereafter.
Safety was assessed during the randomized treatment period by monitoring the frequency, duration, and severity of AEs, including AEs of special interest (AESI; ie, cytopenias, infections, bleeding events, other). AEs were assessed according to the Common Terminology Criteria for Adverse Events v4.03.
Infections were also assessed by investigators using an infection-specific grading system predictive of mortality that was developed for and validated in alloHCT recipients (Cordonnier C, et al. Transplantation. 2006). Infections were classified by type (viral, bacterial, fungal, unknown, other) and severity (grades 1 to 3). We report AEs up to day 28, when exposure to RUX and BAT was similar.
RESULTS
A total of 302 pts (RUX, n = 152; BAT, n = 150) received ≥ 1 dose of study drug and were included in this analysis. Most pts experienced ≥ 1 AE up to day 28, with similar rates observed between RUX (96.1% [grade ≥ 3, 78.3%]) and BAT (94.7% [grade ≥ 3, 79.3%]). The most common AEs (all grades [grade ≥ 3]) in RUX vs BAT pts were thrombocytopenia (32.9% [27.0%] vs 18.7% [16.0%]), anemia (30.3% [22.4%] vs 28.0% [18.7%]), and cytomegalovirus (CMV) infection/reactivation (25.7% [7.2%] vs 20.7% [8.0%]). However, AEs led to low rates of discontinuation (RUX, 11.2%; BAT, 4.0%), primarily due to anemia (2.0% vs 0.7%), thrombocytopenia (2.0% vs 0%), and pancytopenia (1.3% vs 0%).
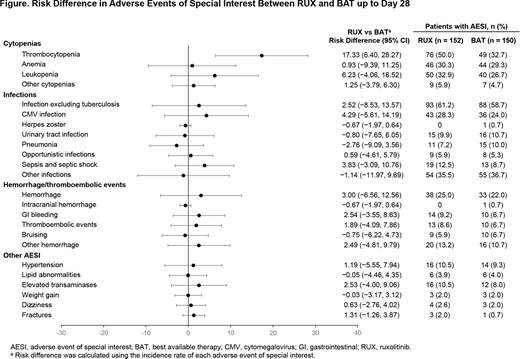
Serious AEs occurred in 37.5% of RUX pts and 34.0% of BAT pts. The most commonly reported serious AEs were sepsis (RUX, 5.3%; BAT, 2.0%), diarrhea (3.3%; 0.7%), and CMV infection/reactivation (2.6%; 3.3%), with sepsis leading to death in 3 RUX pts (2.0%) and 2 BAT pts (1.3%). Among AESI, the most common events were infections excluding tuberculosis (RUX, 61.2% [grade ≥ 3, 32.2%] vs BAT, 58.7% [grade ≥ 3, 37.3%]) and thrombocytopenia (50.0% [41.4%] vs 32.7% [29.3%]). The risk of developing an AESI was similar between RUX and BAT pts, except for the risk of thrombocytopenia, which was higher in pts receiving RUX (Figure). A total of 15 deaths in the RUX arm (9.9%) and 21 in the BAT arm (14.0%) occurred up to day 28. The main cause of death in both arms was aGVHD, with higher rates seen in the BAT arm (11.3% vs 5.9% in the RUX arm).
When assessed using the grading system developed by Cordonnier et al, infections were reported in 61.2% (grade 3, 22.4%) of RUX pts and 55.3% (grade 3, 18.7%) of BAT pts. Among pts with infection, the median time to first occurrence of infection was 2.1 (range, 0-27.0) weeks with RUX vs 1.9 (range, 0-21.3) weeks with BAT. Main types of infections were viral (RUX, 42.8%; BAT, 33.3%), bacterial (29.6%; 32.7%), and fungal (8.6%; 4.7%). The most common viral infections in RUX vs BAT pts were CMV (grade 3, 4.6% vs 3.3%) and Epstein-Barr virus (no grade 3); the most common bacterial infections were urinary tract (no grade 3), device-related (no grade 3), and sepsis (grade 3, 2.6% vs 2.0%); and the most common fungal infections were bronchopulmonary aspergillosis (grade 3, 2.0% vs 0%) and oral candidiasis (no grade 3).
CONCLUSIONS
The safety profile of RUX was consistent with what has been previously reported and what is expected in pts with SR aGVHD, including a higher risk of developing thrombocytopenia with RUX. Up to day 28, the risk of developing other AESI was similar between RUX and BAT. No new or unexpected safety findings were observed.
Von Bubnoff:Novartis: Membership on an entity's Board of Directors or advisory committees, Other: Clinical biomarker research, steering committee, Patents & Royalties: Research support, Research Funding; Astra Zeneca: Honoraria, Other: Lectures, Patents & Royalties: Astra Zeneca. Wagner:MSD: Membership on an entity's Board of Directors or advisory committees; Medac: Other: Travel grand; Shire: Other: Travel grand; Kite/Gilead: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Forcade:JAZZ: Other: Travel grant for congress; NEOVII: Other: Travel grant for congress; Gilead: Speakers Bureau; Novartis: Other: Travel grant for congress; Sanofi: Other: Travel grant for congress. Civriz Bozdag:Novartis: Research Funding. Ayuk:Neovii: Research Funding; Therakos/Mallinckrodt: Honoraria, Research Funding; Kite/Gilead: Honoraria; Celgene: Consultancy, Honoraria; Novartis: Honoraria. Yoon:Amgen: Consultancy, Honoraria; Kyowahako Kirin: Research Funding; Novartis: Consultancy, Honoraria; Janssen: Consultancy; F. Hoffmann-La Roche: Other: All authors received support for third-party writing assistance, furnished by Scott Battle, PhD, provided by F. Hoffmann-La Roche, Basel, Switzerland., Research Funding; YuhanPharma: Research Funding. García Gutiérrez:Novartis Pharma AG: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Incyte: Consultancy, Honoraria, Research Funding; Bristol-Myers Squibb: Consultancy, Honoraria, Research Funding. Rubio:Medac: Consultancy; Gilead: Honoraria; MSD: Honoraria; Novartis: Honoraria; Neovii: Research Funding. Xu:Novartis: Current Employment. Morando:Novartis: Current Employment. Mahuzier:Novartis: Current Employment. Chandraiah:Novartis: Current Employment. Socié:Incyte: Speakers Bureau; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Alexion: Consultancy, Honoraria, Research Funding; Elsalys: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal